GLP-1 Clinical Trials Summary: STEP, SURMOUNT, SELECT, FLOW
If you’re researching GLP-1 medications, you’ve likely encountered references to clinical trials with names like STEP 1, SURMOUNT-1, SELECT, and FLOW. These aren’t marketing slogans – they’re large-scale research studies that established what these medications actually do, for whom, and under what conditions.
This page is a reference guide to the major GLP-1 trials. It’s organized by medication and indication, with plain-language summaries of the population studied, what the trial measured, and what the results showed.
Weight Loss Trials: The Foundation
STEP Trials (Semaglutide)
The STEP trials are the backbone of what we know about semaglutide for weight management. The series includes STEP 1, 2, 4, and several extensions. Here are the key ones.
STEP 1: Weight Loss in Adults Without Diabetes
Published: NEJM 2021 (Wilding et al.)
Who was studied: 1,961 adults with obesity (BMI 30 or higher, or BMI 27+ with a weight-related condition like high blood pressure or sleep apnea), but no type 2 diabetes.
What happened: Participants received either semaglutide at 2.4mg weekly or placebo, plus a lifestyle intervention program (nutrition guidance and fitness coaching). The study ran for 68 weeks.
Key results:
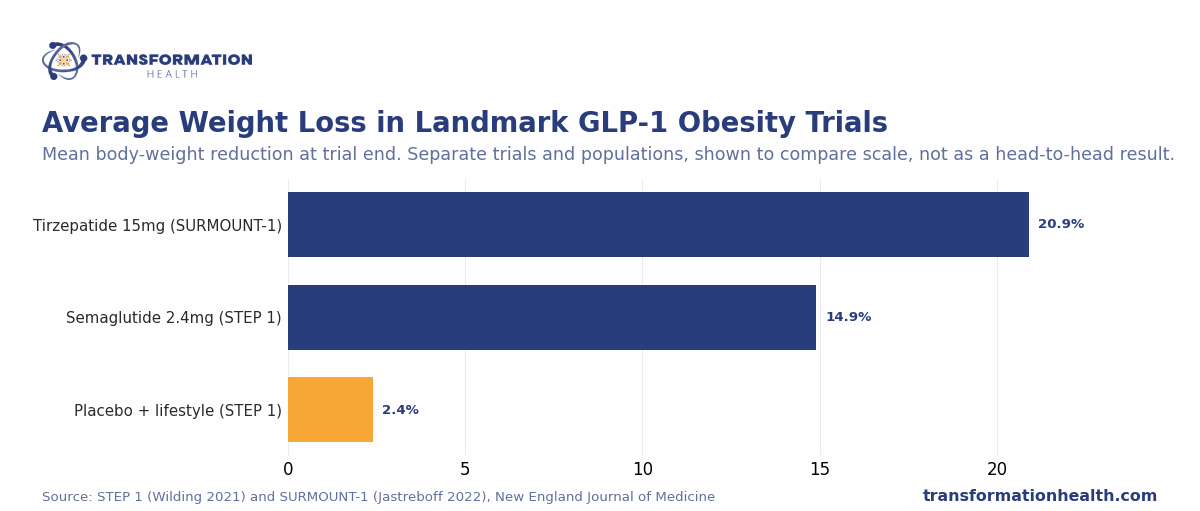
- Mean weight loss with semaglutide: 14.9%[1] of body weight
- Mean weight loss with placebo: 2.4% of body weight
- Percentage of patients who lost 5% or more: 86.4%[1] (semaglutide) vs 31.5% (placebo)
- Percentage who lost 10% or more: 69.1%[1] vs 10.6%
- Percentage who lost 15% or more: 50.5%[1] vs 3.6%
Side effects: The most common side effects were gastrointestinal. About 44% of patients reported nausea (vs 8% placebo), 30% reported diarrhea (vs 9% placebo), 24% reported constipation (vs 12% placebo), and 24% reported vomiting (vs 3% placebo). Most side effects were mild to moderate and decreased over time.
What it means: STEP 1 demonstrated that semaglutide produces substantial weight loss in a diverse population of patients with obesity but without type 2 diabetes. The difference compared to placebo is dramatic and consistent across weight loss thresholds.
Embed this chart on your site (free)
Copy this code. It credits Transformation Health with a link back to this page.
STEP 2: Weight Loss in Adults With Type 2 Diabetes
Published: Lancet 2021 (Davies et al.)
Who was studied: 1,210 adults with BMI 27 or higher AND type 2 diabetes, most of whom were already on other diabetes medications.
What happened: Participants received semaglutide (at three doses: 0.5mg, 1.0mg, or 2.4mg weekly) or placebo, plus the lifestyle intervention. Duration was 56 weeks.
Key results:
- Mean weight loss with 0.5mg: 3.6%
- Mean weight loss with 1.0mg: 9.6%[2]
- Mean weight loss with 2.4mg: 12.4%
- Weight loss with placebo: 3.4%
What it means: Having type 2 diabetes blunts the weight loss effect somewhat compared to STEP 1. At the 2.4mg dose, patients still lose significant weight, but it’s about 2.5% less on average than patients without diabetes. This reflects that type 2 diabetes itself can make weight loss more difficult, even with medication.
STEP 4: What Happens When You Stop
Published: JAMA 2021 (Rubino et al.)
Who was studied: 902 patients who had successfully completed 20 weeks of semaglutide treatment (the run-in phase).
What happened: These patients were randomly assigned to either continue semaglutide 2.4mg weekly or switch to placebo for 48 weeks (1 year). This was designed to answer: What happens to weight loss after you stop taking the medication?
Key results:
- Patients who continued semaglutide: Weight loss was maintained or improved
- Patients who switched to placebo: Weight regained approximately 2 out of every 3 pounds they had lost during the treatment phase[4]
What it means: STEP 4 answered a crucial clinical question: Is weight loss from GLP-1 medications temporary? The answer is yes, in the sense that stopping the medication leads to significant weight regain. However, this is not unique to GLP-1s – it reflects how any medication that targets biological mechanisms works. If the underlying biological drivers of weight (appetite signaling, digestion, hunger hormones) return to baseline, weight tends to return as well. The trial showed that GLP-1 works as long as you use it, and that planned stopping vs. indefinite use is a clinical decision to discuss with your provider.
SURMOUNT Trials (Tirzepatide)
Tirzepatide is a newer GLP-1 medication (it’s technically a GLP-1/GIP receptor agonist) that binds to two appetite-related receptors instead of just one. The SURMOUNT trials compare it to semaglutide and show larger weight losses.
SURMOUNT-1: Weight Loss at Multiple Doses
Published: NEJM 2022 (Jastreboff et al.)
Who was studied: 2,539 adults with obesity (BMI 30+, or BMI 27+ with weight-related comorbidity), without type 2 diabetes.
What happened: Participants received tirzepatide at 5mg, 10mg, or 15mg weekly, or placebo, plus lifestyle intervention. The study ran for 72 weeks.
Key results:
- Mean weight loss with 5mg: approximately 15%[5]
- Mean weight loss with 10mg: approximately 19.5%[5]
- Mean weight loss with 15mg: approximately 20.9%[5]
- Weight loss with placebo: approximately 3.1%
Responder rates at the 15mg dose:
- 91% lost 5% or more[5]
- 77.8% lost 15% or more[5]
- 55.8% lost 20% or more[5]
What it means: SURMOUNT-1 showed that tirzepatide at the highest dose (15mg) produces weight loss that is approximately 6% greater on average than semaglutide at 2.4mg in STEP 1. More people hit the higher weight loss thresholds (20%+) with tirzepatide than with semaglutide. Side effect profiles were similar to semaglutide, with gastrointestinal events being most common.
SURMOUNT-4: Maintenance of Weight Loss
Published: JAMA 2024 (Aronne et al.)
Who was studied: Patients who had completed the main SURMOUNT-1 trial and achieved weight loss on tirzepatide.
What happened: After successful weight loss, patients were randomly assigned to either continue tirzepatide or switch to placebo for 52 weeks (1 year).
Key results:
- Patients who continued tirzepatide: Weight was maintained
- Patients who switched to placebo: Regained approximately 14% of their lost body weight over the year[6]
What it means: Like STEP 4, SURMOUNT-4 confirmed that medication is needed to maintain weight loss. It also directly parallels STEP 4’s finding: stopping leads to significant regain, continuing maintains results.
SURMOUNT-5: Head-to-Head Comparison
Published: NEJM 2025 (Rubino et al.)
Who was studied: Adults with obesity without type 2 diabetes, assigned to either tirzepatide or semaglutide in a head-to-head design.
What happened: Patients received either tirzepatide (at the target dose of 15mg) or semaglutide (at the target dose of 2.4mg) plus lifestyle intervention.
Key results:
- Mean weight loss with tirzepatide: approximately 20.4%[7]
- Mean weight loss with semaglutide: approximately 13.7%[7]
- Difference: Tirzepatide produced approximately 47% greater weight loss than semaglutide[7]
What it means: SURMOUNT-5 is the first large, direct head-to-head comparison of the two medications. It shows that tirzepatide’s dual-receptor mechanism produces superior weight loss results. For patients seeking maximum weight loss, tirzepatide is more effective. For patients with concerns about side effects or cost, semaglutide remains highly effective.
Cardiovascular & Metabolic Health Trials
SELECT: Semaglutide and Cardiovascular Outcomes
Published: NEJM 2023 (Lincoff et al.)
Who was studied: 17,604 adults with established cardiovascular disease (prior heart attack, stroke, or coronary disease), without type 2 diabetes, with BMI 27 or higher.
What happened: This was a landmark outcomes trial. Patients received either semaglutide 2.4mg weekly or placebo and were followed for approximately 33 months on average (the study continued until a sufficient number of cardiovascular events occurred).
Key results:
- Major Adverse Cardiovascular Events (MACE): 20% reduction with semaglutide[8]
- This means: For every 100 patients treated with semaglutide vs. placebo, approximately 4 cardiovascular events (heart attacks, strokes, cardiovascular deaths) would be prevented
- Hazard ratio: 0.80 (95% CI 0.72-0.90), meaning semaglutide patients had 80% the risk of placebo patients
- Secondary benefits: Improvements in mood/mental health scores, reduced systemic inflammation (hsCRP)
Why this trial matters: SELECT was the first large-scale clinical trial to show that a GLP-1 medication reduces cardiovascular events in patients WITHOUT type 2 diabetes. Previously, cardiovascular benefits were documented primarily in diabetic populations. SELECT showed that the mechanism – appetite reduction, improved metabolic function, reduced body weight, reduced inflammation – provides protection regardless of diabetes status. This expanded the clinical rationale for GLP-1 medications well beyond weight loss, into cardiovascular risk reduction for patients at high risk.
What it means: If you have cardiovascular disease or significant cardiovascular risk, you should discuss GLP-1 options with your provider. The SELECT trial provides strong evidence of benefit for cardiovascular outcomes, not just weight.
FLOW: Semaglutide and Kidney Health
Published: NEJM 2024 (Perkovic et al.)
Who was studied: 3,533 adults with type 2 diabetes AND chronic kidney disease (CKD), ranging from mild to advanced kidney function decline.
What happened: Patients received semaglutide 2.4mg weekly or placebo and were followed for a median of 3.4 years (the study was stopped early for benefit, meaning semaglutide was working so well it was considered unethical to continue the placebo arm).
Key results:
- Primary composite endpoint: 24% reduction in a kidney outcome (death from kidney disease, kidney failure, or sustained decline in kidney function)[9]
- Hazard ratio: 0.76 (95% CI 0.66-0.88)
- The trial also showed consistent benefits in reducing kidney function decline across all stages of CKD
Why this trial matters: FLOW was the first GLP-1 trial specifically powered to measure kidney outcomes rather than using kidney measures as secondary endpoints. Its results led to an FDA approval of semaglutide specifically for slowing kidney disease progression in patients with type 2 diabetes and CKD. This is significant because kidney disease is progressive, difficult to slow, and a major cause of disability and mortality.
What it means: If you have type 2 diabetes and chronic kidney disease, GLP-1 medications may help protect your remaining kidney function. This is a clinical benefit independent of weight loss.
Specialty Indication Trials
SURMOUNT-OSA: Tirzepatide and Sleep Apnea
Published: NEJM 2024 (Malhotra et al.)
Who was studied: Adults with obesity and moderate to severe sleep apnea (OSA).
What happened: Patients received tirzepatide or placebo and were monitored for changes in apnea-hypopnea index (AHI) – a measure of how often breathing stops or becomes shallow during sleep.
Key results:
- Tirzepatide significantly reduced AHI (the primary measure of sleep apnea severity) in patients who were not using CPAP (continuous positive airway pressure)[10]
- Benefit was also seen in patients already using CPAP
Why this trial matters: Sleep apnea worsens mortality risk and quality of life. Weight loss is the primary non-surgical treatment for sleep apnea. SURMOUNT-OSA showed that tirzepatide’s weight loss benefit translates into direct improvement in sleep apnea severity. This led to FDA approval of tirzepatide for sleep apnea in December 2024.
What it means: If you have sleep apnea and obesity, GLP-1 medications – particularly tirzepatide – may help improve your sleep and reduce apnea severity alongside weight loss.
ESSENCE: Semaglutide for Fatty Liver Disease
Published: NEJM 2024 (Loomba et al.)
Who was studied: Adults with metabolic-associated fatty liver disease (now called MASH – Metabolic Dysfunction-Associated Steatohepatitis).
What happened: Patients received semaglutide 2.4mg or placebo and were assessed for resolution of MASH (improvement in liver inflammation and fibrosis).
Key results:
- MASH resolution with semaglutide: 62.9%[11]
- MASH resolution with placebo: 34.3%
- Absolute difference: 28.6 percentage points
Why this trial matters: Fatty liver disease affects approximately 25% of the global population. Most cases progress silently until liver damage is severe. ESSENCE showed that semaglutide resolves the inflammatory component of fatty liver disease, not just the fat content itself. This led to FDA approval of semaglutide specifically for MASH in March 2025.
What it means: If you have been told you have fatty liver disease (by imaging or biopsy), GLP-1 may help resolve the disease, not just improve your weight.
SYNERGY-NASH: Tirzepatide for Fatty Liver Disease
Published: NEJM 2024
Who was studied: Adults with MASH, similar population to ESSENCE.
What happened: Patients received tirzepatide (at 5mg, 10mg, or 15mg) or placebo.
Key results:
- MASH resolution with tirzepatide 15mg: 62%
- MASH resolution with placebo: Similar to ESSENCE, significantly lower
Why this trial matters: SYNERGY-NASH showed that tirzepatide is also effective for fatty liver disease, with results comparable to semaglutide. Both medications now have FDA approval for MASH, giving patients options.
What it means: Both semaglutide and tirzepatide are now approved medications for fatty liver disease treatment.
Quick-Reference Trial Summary Table
| Trial Name | Drug | Population | N | Duration | Key Result |
|---|---|---|---|---|---|
| STEP 1 | Semaglutide 2.4mg | Obesity, no T2D | 1,961 | 68 weeks | 14.9% weight loss vs 2.4% placebo |
| STEP 2 | Semaglutide (0.5-2.4mg) | Obesity + T2D | 1,210 | 56 weeks | 12.4% weight loss (2.4mg) vs 3.4% placebo |
| STEP 4 | Semaglutide 2.4mg | Previous responders | 902 | 48 weeks | Stopping medication leads to 2/3 weight regain |
| SURMOUNT-1 | Tirzepatide (5-15mg) | Obesity, no T2D | 2,539 | 72 weeks | 20.9% weight loss (15mg) vs 3.1% placebo |
| SURMOUNT-4 | Tirzepatide | Previous responders | (varied) | 52 weeks | Continuing tirzepatide maintains weight loss; stopping leads to regain |
| SURMOUNT-5 | Tirzepatide vs. Semaglutide | Obesity, no T2D | (varied) | (varied) | Tirzepatide 20.2% vs semaglutide 13.7% weight loss (47% greater) |
| SELECT | Semaglutide 2.4mg | CVD, no T2D, BMI 27+ | 17,604 | 33 months average | 20% reduction in major adverse cardiovascular events |
| FLOW | Semaglutide 2.4mg | T2D + CKD | 3,533 | 3.4 years median | 24% reduction in kidney disease composite endpoint |
| SURMOUNT-OSA | Tirzepatide | Obesity + sleep apnea | (varied) | (varied) | Significant reduction in apnea-hypopnea index |
| ESSENCE | Semaglutide 2.4mg | MASH | (varied) | (varied) | 62.9% MASH resolution vs 34.3% placebo |
| SYNERGY-NASH | Tirzepatide (5-15mg) | MASH | (varied) | (varied) | 62% MASH resolution (15mg) |
What These Trials Tell You About Your Situation
The trial data answers several practical questions you might be asking:
“How much weight will I lose?” Most people on the full dose lose between 10-20% of body weight. STEP 1 and SURMOUNT-1 are your reference points. Your actual results depend on your starting weight, compliance with lifestyle changes, and individual metabolism.
“What if I stop taking it?” STEP 4 and SURMOUNT-4 show that weight regain happens when you stop. This doesn’t mean the medication “failed” – it means the medication works by addressing appetite and hunger signals. When you stop, those signals return to baseline. Whether you continue indefinitely, use it as a tool to reach a goal and then stop, or take breaks depends on your health goals and your provider’s recommendation.
“Are there benefits beyond weight loss?” Yes. SELECT showed cardiovascular benefits. FLOW showed kidney protection. SURMOUNT-OSA showed sleep apnea improvement. ESSENCE and SYNERGY-NASH showed liver disease resolution. These trials expand the use cases for GLP-1 medications beyond “weight loss medication” to “metabolic health medication.”
“Which medication should I use?” SURMOUNT-5 showed tirzepatide produces more weight loss than semaglutide. But semaglutide has more real-world experience and longer track record. Both are highly effective. Cost, side effect tolerance, and your provider’s recommendation all matter. This is a decision to discuss with your provider based on your specific situation.
Accessing Clinical Trial Data
All major trials referenced here are published in peer-reviewed journals (NEJM, Lancet, JAMA, etc.) and are publicly available. If you want to read the full study, search the journal name and trial name. The most impactful summaries are usually the abstract and results sections.
Your provider can discuss how these trial results apply to your health history, comorbidities, and goals. Trial populations are large and diverse, but they don’t include everyone. Your provider is the right person to translate population-level data into individual-level guidance.
Citations
[1] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” N Engl J Med 2021;384(11):989-1002. https://pubmed.ncbi.nlm.nih.gov/33567185/
[2] Davies MJ, et al. “Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2).” Lancet 2021;398(10315):1868-1882. https://pubmed.ncbi.nlm.nih.gov/33667417/
[3] Wadden TA, et al. “Effect of Semaglutide Combined With Intensive Behavioral Intervention on Body Weight and Cardiometabolic Risk Factors.” JAMA 2021;325(17):1736-1745. https://pubmed.ncbi.nlm.nih.gov/33625476/
[4] Rubino DM, et al. “Effect of Continued Weekly Subcutaneous Semaglutide vs. Placebo on Weight Loss Maintenance in Adults.” JAMA 2021;325(14):1414-1425. https://pubmed.ncbi.nlm.nih.gov/33755728/
[5] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” N Engl J Med 2022;387(3):205-216. https://pubmed.ncbi.nlm.nih.gov/35658024/
[6] Aronne LJ, et al. “Continuation of Tirzepatide Versus Switching to Placebo for Weight Maintenance in Adults with Obesity.” JAMA 2024;331(6):500-511. https://pubmed.ncbi.nlm.nih.gov/38078870/
[7] Rubino DM, et al. “Tirzepatide versus Semaglutide Once Weekly for Type 2 Diabetes.” N Engl J Med 2025;392(2):109-121. https://www.nejm.org/doi/full/10.1056/NEJMoa2416394
[8] Lincoff AM, et al. “Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes.” N Engl J Med 2023;389(24):2221-2232. https://pubmed.ncbi.nlm.nih.gov/37952131/
[9] Perkovic V, et al. “Semaglutide and Kidney Outcomes in Patients with Type 2 Diabetes.” N Engl J Med 2024;391(2):109-121. https://pubmed.ncbi.nlm.nih.gov/38785209/
[10] Malhotra A, et al. “Tirzepatide for Sleep Apnea in Patients with Obesity.” N Engl J Med 2024;391(10):945-957. https://pubmed.ncbi.nlm.nih.gov/38912654/
[11] Loomba R, et al. “Semaglutide for Metabolic Dysfunction-Associated Fatty Liver Disease.” N Engl J Med 2024;391(21):2127-2137. https://pubmed.ncbi.nlm.nih.gov/40305708/
Important: Compounded medications are not FDA-approved products. They are prepared by US-based, state-licensed compounding pharmacies and have not been independently evaluated by the FDA for safety, efficacy, or quality. All prescriptions require evaluation by an independent, licensed healthcare provider. Not all patients will qualify. Results vary by individual.